Overview, Signs and Symptoms of an Obstruction
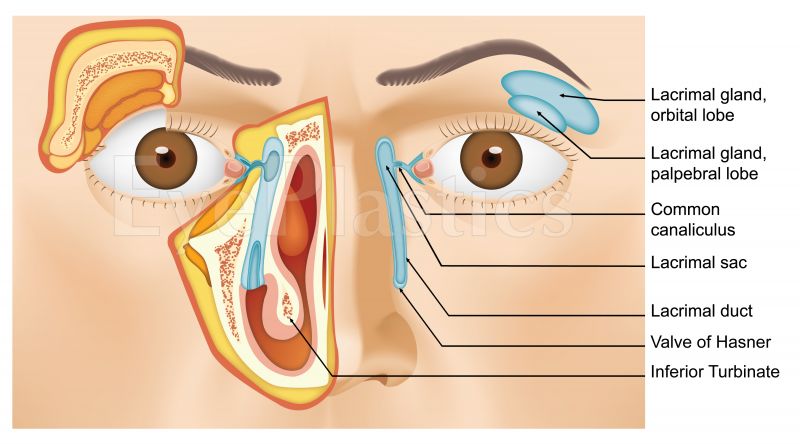
- The lacrimal gland produces tears which enter into the "duct"
that drain the tears from the eye into the nose. The most common symptoms are If one has a plugged up "tear duct," not only will tears spill over the eyelids and
run down the face, but the stagnant tears within the system can become infected.
- (1) excess tearing (tears may possibly run down the face) and
- (2) mucous discharge
- This may possibly lead to recurrent red eyes and infections.
- The excessive tearing can also produce secondary skin changes on the lower eyelids.
Congenital Nasolacrimal Duct Obstruction
The nasolacrimal duct is a duct that connects the lacrimal glands in the eye to the nasal cavity. In this article, we shall briefly review the epidemiology, clinical presentation and the common causes of this condition.
Epidemiology
- Clinical research has shown that nasolacrimal duct obstruction occurs in 2 to 4 out of 100 newborn babies. However, this number dramatically increases in children who have Down syndrome with statistics suggesting about 22% to 36% developing this condition.
- There are a number of different reasons why nasolacrimal duct obstruction occurs. The epidemiological statistics have shown that of all the cases, 35% of them actually due to obstruction, 15% occur due to the improper formation of the opening of the lacrimal duct (punctual agenesis), 10% have some form of abnormal connection i.e. congenital fistula and 5% have defects in the structure of the head and face.
- As such, congenital nasolacrimal duct obstruction does not differentiate between race and sex. It is typically seen in newborns.
- Congenital nasolacrimal duct obstruction can lead to in numerous clinical presentations. These conditions bring with them a varying degree of morbidity and mortality.
- The originally condition that may possibly occur is amniotocoele. Here, there is distension of the tear producing gland i.e. the lacrimal gland. Amniotic fluid enters the lacrimal sac and gets trapped within it. This can lead to in swelling of the lacrimal sac. Treating this can be done through inserting a small probe through the nasolacrimal duct.
- Dacrocystitis is another condition that may possibly develop where there is inflammation and distension of the lacrimal sac. It occurs in the neonatal period which is just after the baby has been born. In these patients as well, probing the lacrimal sac through the nasolacrimal duct is the treatment.
- Finally, in newborns who have narrowing of the nasolacrimal duct, accumulation of pus or pus within the lacrimal sac may possibly take place. This can manifest as constant watering of the eye or expulsion of pus from the eye. The treatment usually involves antibiotics, compression and massage of the lacrimal sac. If left untreated, newborns may possibly have matted eyes every morning and excessive tearing of the eyes.
 |
simple obstruction |
| congenital fistula (as seen to the left) |
| acute dacryocystitis |
| congenital dacryocele or mucocele |
Clinical presentation
- History forms an important part of making a diagnosis. There may possibly be a family history of nasolacrimal duct problems and other abnormalities such as glaucoma. A detailed examination of the eye is useful in determining whether the patient has congenital nasolacrimal duct disease.
- A special test known as the dye disappearance test is useful in determining whether there is any obstruction. In adds to, tests to ascertain whether the patient has glaucoma need to be conducted.
Causes
Nasolacrimal duct obstruction is not very common but does have some recognised causes. The top three causes include –
- genetic causes i.e. having a family history of nasolacrimal duct obstruction
- premature birth
- drug use by the mother during pregnancy
It is commonly accompanied by other eye abnormalities.
Treatment
- 9 out of 10 cases resolve within the originally year of life. If required, massage therapy over the lacrimal gland may possibly be helpful.
- In patients in whom this does not work, using a probe can cure up to 95% of cases. Other procedures include the insertion of a tube into the nasolacrimal gland or the insertion of a balloon catheter.
- Special surgical procedures include a dacrocystorhinostomy - a procedure that helps restore normal tear flow.
Acquired (ADULT-ONSET) Nasolacrimal Duct Obstruction
Epiphora is the overflow of tears which is caused by an imbalance in tear production and tear drainage. Other than conditions that cause an abnormal increase in tear production, an abnormality in tear drainage is the most likely cause of epiphora. It may possibly be either functional due to a displaced punctum, eyelid laxity, weak orbicularis, or facial nerve palsy or an anatomical obstruction may possibly block the drainage of tears. Anatomical obstruction of the nasolacrimal duct may possibly be congenital which occurs during the neonatal period or acquired which manifests during adulthood.
Classification of Acquired Nasolacrimal Drainage Obstruction (NLDO)
Acquired nasolacrimal drainage obstruction may possibly be primary or secondary.
- Primary acquired nasolacrimal drainage obstruction (PANDO) is caused by inflammation or fibrosis without any precipitating cause. The name was given by Linberg and McCormick in 1986.
- Secondary acquired lacrimal drainage obstruction (SALDO) is further classified further based on aetiology as infectious, inflammatory, neoplastic, traumatic and mechanical. This classification was proposed by Bartley.
Pathophysiology/Statistics
- Although quite common, the frequency of nasolacrimal drainage obstruction is unknown. It has no racial predilection.
- PANDO is more commonly seen in middle-aged and elderly females. This is due to the significantly smaller dimensions in the lower nasolacrimal fossa and middle nasolacrimal duct among women. Middle-aged women exhibit alterations in the dimensions of the bony nasolacrimal canal that coincides with osteoporotic changes elsewhere in the body, which supports the higher incidence of PANDO in women. Some suggest that sudden hormonal changes incite generalized de-epithelialization predisposing a narrow duct to be blocked by sloughed off debris.
- SALDO is aetiologically classified as infectious, inflammatory, neoplastic, traumatic, and mechanical.
- Infectious lacrimal drainage obstruction: Bacteria, viruses, fungi, and parasites that have all been implicated are as follows:
- Bacterial Causes – Most common causes are Actinomyces, Propionibacterium, Fusobacterium, Bacteroides, Mycobacterium, and Chlamydia.
- Viral Causes – Most commonly Herpes virus. Due to canalicular obstruction and damage.
- Fungal Causes - Aspergillus, Candida, Pityrosporum, and Trichophyton. Usually cause obstruction due to dacryolith/stone or cast formation.
- Parasitic Causes – Rare but can be caused by Ascaris lumbricoides entering through the valve of Hasner.
Inflammatory lacrimal drainage obstruction: May be endogenous or exogenous in origin.
- Endogenous Causes – Most commonly due to Wegener granulomatosis and sarcoidosis. Other causes include cicatricial pemphigoid, sinus histiocytosis, Kawasaki disease, and scleroderma.
- Exogenous Causes – Eye drops, radiation, systemic chemotherapy, and bone marrow transplantation all cause punctal and canalicular scarring, stenosis and occlusion in varying degrees.
Neoplastic lacrimal drainage obstruction: Neoplasms cause obstruction by primary growth, secondary spread, or metastatic spread.
Traumatic lacrimal drainage obstruction: May be iatrogenic or non-iatrogenic.
- atrogenic Causes - Trauma and subsequent scarring due to overenthusiastic lacrimal probing, orbital decompression surgery, paranasal, nasal, and craniofacial surgery all cause obstruction.
- Non-iatrogenic Causes - Either blunt or sharp injury to the canaliculus, lacrimal sac, and nasolacrimal duct results in post-traumatic dacryostenosis.
Mechanical lacrimal drainage obstruction
- Intraluminal foreign bodies – Dacryoliths or casts due to infection or long-term use of topical medications.
- External compression – Due to rhinoliths, nasal foreign bodies, or mucoceles. Dentigerous cyst in the maxillary sinus is also thought of as a culprit.
Symptoms/Presentation
- Patients with NLDO most commonly present with epiphora, mucoid or purulent discharge with a painful, swollen medical canthus. They often have features of recurrent dacryocystitis, recurrent conjunctivitis, or ocular pemphigus. Some cases present with bloody tears and even epistaxis as in nasal, sinus or lacrimal sac tumours.
- A thorough past ocular and medical history is in order to evaluate the cause of the disease. Always ask for previous eye surgery, lid surgery, use of antiglaucoma medications, or any other topical medications. Past medical history should all causes cited in the previous section.
On examination, the following findings may possibly be present.
- Gross observation shows overflowing tears, fluctuant tender mass over medial canthus, mucoid or purulent eye discharge. Regurgitation test results in mucoid reflux with lacrimal massage indicating lower system obstruction.
- Slit lamp examination shows enhancement of tear meniscus height by fluorescein greater than 2 mm, punctal stenosis, canaliculitis, concretions expressed from the punctum
Investigations
- Laboratory studies include sending lacrimal discharge for Gram/Giemsa stain, culture and sensitivity, KOH and anticytoplasmic antibodies.
- Imaging studies may possibly include dacryocystography, dacryoscintigraphy, CT scan, CT dacryocystography (CTDCG), nasal endoscopy, or Gadolinium-enhanced magnetic resonance dacryocystography.
- Other tests include Schirmer test, Fluorescein dye disappearance test, lacrimal irrigation, probing of the canaliculi, Jones dye tests, microreflux test, Hornblass saccharine test
- Diagnostic canalicular irrigation determines the level of canalicular obstruction staging it as partial obstruction, total common canalicular obstruction, total functional occlusion and complete nasolacrimal obstruction.
Treatment
Medical Care
- Topical antibiotics in early infections
- Systemic antibiotics in chronic or severe infections
Surgical Care
- External dacryocystorhinostomy
- Endoscopic mechanical/nonlaser dacryocystorhinostomy
- Endoscopic laser dacryocystorhinostomy
- Endoscopic laser-assisted dacryocystorhinostomy
- Conjunctivodacryocystorhinostomy (CDCR)
- Balloon catheter dilatation
- Inferior meatus surgery
  |
The photo and CT on the left represents a nasolacrimal duct tumor which can lead to in a nasolacrimal duct obstruction.
Once the tumor was removed, silicone intubation performed, the patient's symptoms of tearing resolved
|


